|
|
|
|
|
|
#10-16 Connexion Farrer Park
Medical Centre
1 Farrer Park Station Road
Singapore 217562
[getting there]
|
|
|
|
|
|
| Phone : | +65 67330846 | | Fax : | +65 67330849 | 24Hr Answering
Service : | +65 65358833 |
|
|
|
|
|
|
| Mon - Fri : | 9:00am - 5:00pm | | Sat : | 9:00am - 1:00pm |
|
|
|
|
|
|
|
Cancer Surgery: Gastric (Stomach) Cancer
|
Gastric (stomach) cancer is a disease where malignant (cancer) cells arise from the lining of the stomach. Gastric cancers are classified according to cell type: the most common type of gastric cancer is adenocarcinoma, which consists of cells arising from glands in the lining of the stomach.
The rest of the information presented here will refer specifically to gastric adenocarcinoma.
Trends in Gastric Cancer Incidence
Overall, the incidence of gastric cancer worldwide has fallen dramatically over the past 70 years. Despite this recent decline, gastric cancer remains the 4th most common cancer and the second leading cause of cancer-related death in the world. A similar decreasing trend in incidence has been noted in Singapore. Even so, gastric cancer remains a significant health problem in the local population: gastric cancer is the 4th and 6th most common cancer among Singapore men and women respectively.
Geographical Variation in Gastric Cancer Incidence
|
|
|
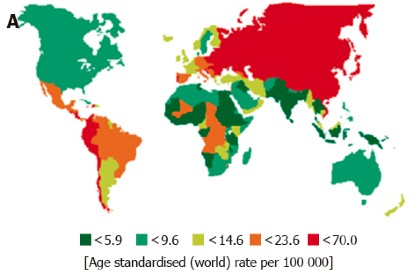
Parkin DM. International variation. Oncogene 2004; 23: 6329-6340
|
Gastric cancer incidence rates vary by up to 10 times throughout the world. The graphic above shows this wide variation from one country to another. Gastric cancer ‘hot spots’ are shown in red. Japan and Korea have some of the highest rates of gastric cancer in the world. Consequently Japanese & Korean surgeons have the greatest experience and arguably, the best results in treating gastric cancer. For this reason, Dr Eric Gan chose to train in gastric surgery at the National Cancer Center in Tokyo, a leading centre for gastric cancer surgery.
It is interesting to note that migrant populations from high-risk areas such as Japan show a marked reduction in gastric cancer risk when they move to low-incidence regions such as the US. Subsequent generations of Japanese migrants acquire risk levels approximating those of the host country.
What causes stomach cancer?
Doctors are uncertain about the exact cause of gastric cancer. Like many other cancers, there are probably multiple factors involved. The marked geographical variation and the effect of migration on gastric cancer risk suggest that environmental and lifestyle factors are important contributors to this disease. Some risk factors have been identified including:
|
- Helicobacter pylori infection. Infection of the stomach with this bacteria may cause chronic inflammation of the stomach lining leading to precancerous changes. H pylori infection is considered a risk factor for gastric cancer.
- Diet. A diet high in smoked or salt-preserved foods such as smoked fish/ meat and pickled vegetables has been shown to be associated with a higher risk of developing gastric cancer. Conversely, a diet that is high in fresh fruits and vegetables may decrease this risk.
- Obesity. This has been identified as a risk factor for cancer affecting the upper part of the stomach.
- Race. Gastric cancer is more common in Asians than Caucasians.
- Gender. Gastric cancer is more common in men than women.
- Age. Gastric cancer is usually seen in people age > 60.
- Previous stomach surgery. Individuals who have had parts of their stomach removed have an increased risk of developing gastric cancer in the remaining stomach.
|
What are the symptoms of stomach cancer?
These include:
|
- Pain or discomfort in the ‘stomach region’ or upper abdomen
- Bloating discomfort after eating
- Passing black stool
- Anaemia
- Unexplained weight loss and loss of appetite
- Heartburn
|
How is stomach cancer diagnosed?
Some abnormalities may be detected by your doctor during physical examination. However, abnormalities detected on abdominal examination by your doctor usually indicate advanced tumour stage.
It is best to consult a doctor early should you experience any of the symptoms listed above. If your symptoms are persistent your doctor may refer you for a test known as gastroscopy. A thin, lighted tube with a miniature video camera called a gastroscope is passed from the mouth into the stomach. High resolution optics allow a detailed examination of the inside of the stomach. If an abnormal area is seen, the doctor will remove some tissue for testing. This is the only way to confirm gastric cancer.
Stomach cancer staging
Once a diagnosis of stomach cancer is made, the next step is to determine how far the cancer may have invaded through the layers of the stomach, and whether the cancer has spread to involve nearby lymph nodes and other organs. This process is called staging and is important in helping us decide which form of treatment would be suitable in each individual patient.
Staging for stomach cancer may involve one or more of the following tests:
|
- Endoscopic ultrasound (EUS). A specially designed gastroscope with an ultrasound probe attached to its tip is used to bounce sound waves off the walls of the stomach. Because the gastroscope allows the doctor to bring the ultrasound probe right next to the cancer, highly detailed images of the tumour and the different layers of the stomach wall and surrounding structures, including lymph nodes may be obtained.
- Computed tomography (CT). These are X-ray scanners which provide images which help determine extent of tumour spread.
- Laparoscopy. In some cases, doctors may use minimally invasive surgical techniques to stage stomach cancer. A small incision is made near the belly button which will allow the surgeon to insert a thin, lighted telescope (‘laparoscope’) into the abdominal cavity. The telescope is connected to high resolution video screens allowing inspection of the abdominal cavity, the outside wall of the stomach, lymph nodes and surrounding organs. Samples may be obtained from suspicious areas to determine tumour spread.
|
How is stomach cancer treated?
Treatment depends on the stage of the cancer. We will devise an individualized treatment plan based on information from one or more of the tests described above. Treatment for stomach cancer may involve endoscopic removal, surgery, chemotherapy, radiotherapy or a combination of these.
Endoscopic removal
This form of treatment is appropriate only for early, small cancers which have not invaded beyond the innermost layers of the stomach wall. Fewer than 10% of gastric cancers diagnosed in Singapore are found at this early stage. Removal of these early cancers may be performed through a gastroscope: the surgeon uses special tools to remove the cancer with a margin of healthy, non-cancerous tissue. This procedure is performed in an endoscopy suite and general anaesthesia is not required.
Surgery for Gastric Cancer
Surgery is a critical part of the treatment plan for many patients with gastric cancer.
We believe that radical gastric surgery with systematic removal of lymph nodes draining the stomach (D2 dissection) is important in improving outcome for gastric cancer. This is a technique originally developed by Japanese gastric cancer surgeons in an effort to improve treatment results for gastric cancer.
Admittedly, there is controversy in the medical literature regarding the role of extended lymph node removal (D2 dissection) in gastric cancer surgery. Several multicentre clinical trials from Western countries have failed to duplicate the excellent results achieved by Japanese centres. This may be partially due to the lower volume of gastric cancer surgery performed in Western centres as gastric cancer is much less common in Caucasian populations.
Having said this, many tertiary referral centres in Western countries have adopted Japanese techniques for gastric cancer surgery.
|
Minimally Invasive Gastric Surgery
In selected cases, minimally invasive techniques may be used to remove stomach cancer. During these procedures, a thin, lighted tube with a video camera at its tip is inserted through a tiny incision near the belly button. This camera is connected to a high-resolution video monitor and provides a magnified, high-resolution image of the abdominal cavity. Guided by this magnified image, we operate to remove the stomach through tiny surgical ‘ports’ using specially designed instruments.
|
Combination (Multimodality) Therapy for Gastric Cancer
Recent studies suggest that for patients at high risk for recurrence of stomach cancer, treatment using a combination of surgery, chemotherapy and/or radiotherapy may improve survival compared to surgery alone.
Two approaches have been described in major clinical trials:
|
- One approach is to use ‘perioperative chemotherapy’ where chemotherapy is given both prior to and after surgery. [1]
- Another approach is to use combination chemotherapy and radiation therapy after surgery [2].
|
- D. Cunningham, W. H. Allum, S. P. Stenning, J. N. Thompson, C. J. Van de Velde, M. Nicolson, J. H. Scarffe, F. J. Lofts, S. J. Falk, T. J. Iveson, D. B. Smith, R. E. Langley, M. Verma, S. Weeden, and Y. J. Chua, for the MAGIC Trial Participants, Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer, New England Journal of Medicine 355(1), 2006: 11-20
- J. S. Macdonald, S. R. Smalley, J. Benedetti, S. A. Hundahl, N. C. Estes, G. N. Stemmermann, D. G. Haller, J. A. Ajani, L. L. Gunderson, J. M. Jessup, and J. A. Martenson, Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction, New England Journal of Medicine 345(10), 2001: 725-30.
|
|